Abstract
Source: Zhang, G., et al. Identification and Characterization of Metastatic Factors by Gene Transfer into the Novel RIP-Tag; RIP-tva Murine Model. J. Vis. Exp. (2017)
This video describes the protocol for intracardiac injection of retroviruses into the transgenic mouse to ensure gene transfer into proliferating pancreatic β premalignant lesions. This method can also help in assessing the functions of candidate genes in tumor metastasis.
Protocol
All procedures involving animal models have been reviewed by the local institutional animal care committee and the jove veterinary review board.
1. Intracardiac injection:
Hemizygous RIP-Tag mice, not homozygous mice, are used in this study. Hemizygous RIP-Tag mice develop pancreatic neuroendocrine tumors around 10~12 weeks of age, while homozygous mice have a shorter tumor latency. Because cell proliferation is required for the incorporation of the viral cDNA into the host genome, 7-week-old RIP-Tag; RIP-tva mice with hyperplasic pancreatic β cells are used. Please note that most normal β cells are not proliferating in adult mice.
- Use 7 week-old RIP-Tag; RIP-tva mice in a pure C57BL/C background for the experiments.
- Anesthetize mouse using a ketamine/xylazine combination (150 mg/kg; 15 mg/kg). Use heat support to maintain the mouse body temperature throughout the entire period of anesthesia.
- Apply eye lubricant to both eyes to prevent corneal drying.
- Shave hair from the chest cavity of RIP-Tag; RIP-tva mice. Position mouse on its back with chest facing up. A toe-pinch is performed to observe the animal for non-responsiveness to confirm full anesthesia effect.
- Extend the front limb and secure them with tapes. Mark mouse's chest for injection. Mark a location midway between the sternal notch and top of xiphoid process, and slightly left (anatomical) of the sternum (Figure 1).
- Scrub the anterior chest wall with either a povidone-iodine scrub or a chlorhexidine scrub followed by a 70% isopropyl alcohol or 70% ethanol soaked gauze sponge.
- Draw 50 µl of air into a sterile 28 g ½ insulin syringe to create space between the plunger and meniscus of a 500 µL syringe, and then draw up 100 µl of viruses. The air space without any liquid on the wall is crucial for seeing cardiac pulse.
- Keep needle upright. Hold skin of mouse taut with one hand, and insert needle to the marked location. When a bright red pulse of blood appears in the syringe, stop advancing the needle and fix the depth of the needle in the mouse with one hand.
- Use the other hand to carefully and slowly push the plunger to deliver viral suspension (~100 µl volume) over a ~60 second period. Deliver 10-20 µl whenever seeing a bright red pulse of blood appear in the syringe. Continuous entrance of red oxygenated blood into the transparent needle hub indicates proper positioning of the needle into the left ventricle.
- After the last push of the plunger to deliver viral suspension and before seeing the next red pulse of blood, quickly retract the needle out of the chest cavity.
- Apply gentle pressure over the injection site to reduce bleeding for at least 1 min.
- Carefully move the mouse onto a heating pad or under a heat lamp until fully conscious. Mice will be watched until anesthesia wears off so that they can walk away from stimuli, a period usually lasting approximately one hour. Mice will be monitored daily for even and intact coat and any changes in behavior.
Representative Results
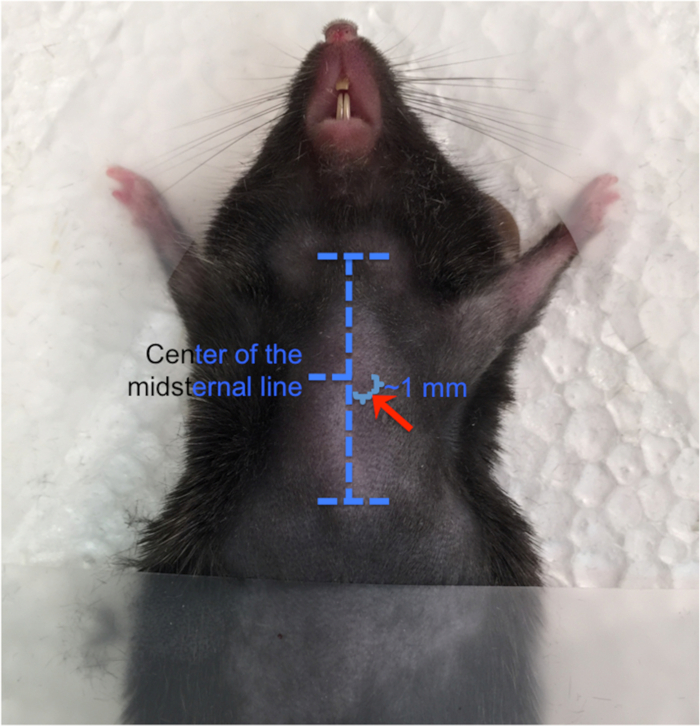
Figure 1: Placement of intracardiac injection. Anatomical landmarks are shown with horizontal dashed lines on the sternum (outlined in white). On the mouse's skin, the sternal notch and xiphoid process serve as landmarks, and the needle is inserted 1 mm away from the mid-sternum and slightly left (anatomical) of the sternum. Please click here to view a larger version of this figure.
Disclosures
No conflicts of interest declared.Materials
| Name | Company | Catalog Number | Comments |
|---|